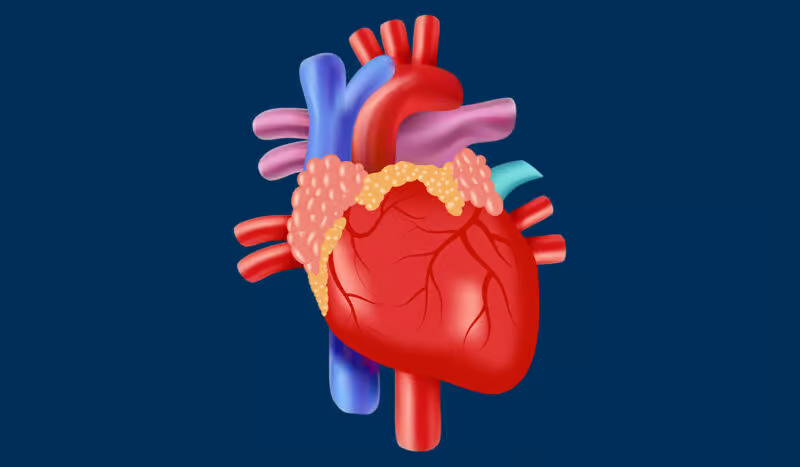
Most commonly, it is caused by a decrease in the flow of blood to the heart. It is a result of the narrowing of the coronary artery. Some patients report it as a digestive issue. Others say the pain goes to the shoulder, arm, neck, or jaw. It is essential to detect angina at an early stage. It could be a warning of a more severe heart event such as a heart attack.
Patients with frequent angina may use activities and medications to control the symptoms, but this does not remove the risk. Control is achievable only after an in-depth understanding of the disease of angina.

Angina is still an important condition in everyday cardiovascular life. In high-income countries, the prevalence of stable angina is static, being around three to four percent for adults over forty.
The number of people suffering from angina is increasing with age. It is particularly high in people with diabetes, high blood pressure, or who are smokers. In low- and middle-income countries, bad diets, intake of drugs, and sedentary lifestyles have increased the incidence of angina and coronary artery diseases in general.
Generally, men appear to be the ones to develop the condition first. However, as women approach menopause, the risk becomes almost equal. Many cases remain hidden because of the mild or irregular representation.
The leading cause of angina is the formation of atherosclerotic plaques in the coronary arteries. Plaque that has a high level of lipid, catheter, and vessel build-up narrows down the lumen of the vessel, and therefore, the amount of blood passing through to feed the heart becomes greatly reduced.
Physical activity or stress may be the factors that lead to the excessive demand for energy. It may cause the chest pain as a result of the lack of supply. Additionally, the plaque that ruptures can also lead to the formation of a blood clot in the lumen. This, in turn, can lead to a more serious condition called unstable angina.
During variant angina, even without major plaque, a constraint in coronary blood flow might result from transient spasms of the vessel. Furthermore, in addition to the aforesaid, micro-vascular dysfunction especially in women is also an essential contributor where small intramyocardial vessels have a problem in dilating. The offset of factors like severe anemia and/or tachyarrhythmias will lead to an increase in the number of persons who experience angina pectoris due to the demand-supply balance being disordered.

The classification is based on the mechanism and the presentation of angina.
Stable angina symptomatically appears when the chest of an angina patient has predictable pain at specific levels of exertion, and severity is diminished when they are given rest or nitrates.
Unstable angina, on the other hand, occurs not only at rest but can also manifest with minimal activity that includes the risk of infarction. This comes along with increased frequency even during the same activities. It also has worsening symptoms like that in the case of infarction.
In variant angina, the person suffering from it may be found undergoing coronary artery spasm. It is the main cause of initiating it. Any of the various forms of angina may initially seem to be a simple or less severe condition. However, the damage made to the heart is almost the same. A heart attack that is considered minor would still be a heart attack that might be complicated by future problems.
The main symptom of angina is pain in the center of the chest. It is often described as pressure, constriction, burning, or tightness. It can travel to the left shoulder, arm, neck, jaw, or back. Some patients compare it to heartburn or dyspepsia, which leads them to an erroneous diagnosis.
Typically, in the case of stable angina, the pain starts with specific reasons such as exercise or emotional stress and then it stops quickly by resting or using sublingual nitrates. Indications of the onset of angina may include shortness of breath, sweating, nausea, and fatigue. Atypical symptoms of angina achievable without chest pain such as jaw pain, epigastric pain, or general weakness are commonly manifested and are most prevalent in the elderly, women, and diabetic patients.
Silent heart ischemia which refers to the situation where a patient does not feel any pain while his ECG shows changes or ischemia marks on imaging is a clear indication of the necessity of objective testing in high-risk groups.
Angina that goes untreated might indicate more serious problems. Unstable angina usually comes before myocardial infarction. This is through the sudden rupture of the plaque in the coronary artery or the formation of a blood clot that blocks the artery. When there are repeated ischemic events, the latter might weaken and destabilize the myocardial muscle, leading to a possible situation of left ventricular dysfunction and heart failure.
Chronic ischemia could also be the cause of arrhythmias, including dangerous ventricular tachycardias. During spasms, variant angina can cause an electrical disturbance that may result in dangerous heart rhythms. Silent ischemia is related to the fact that sometimes, patients experience recorded episodes of painless myocardial injury. Fear of repeated chest pain episodes can be a major reason for the deterioration of the patients' health resulting in anxiety, the lack of desire to do physical activities, and depression.
The latter can be a key factor for psychological disturbances that might compromise an individual's overall health, leading to lower exercise capacity and increased risk of having an ischemic heart attack.
The first step in evaluating angina is to take a detailed medical history of the person's chest pain problem. That includes pain duration, situation of pain, triggers, and relief factors. Also, doctors should run some cardiovascular tests and know the cardiovascular risk factors for a patient like high blood pressure, diabetes, smoking, and family history.
ECG is the basic screening test. The ST segment depression and T wave inversion are the two kinds of abnormalities that can occur during a painful exit of electricity from the chest muscle and such events can point to the ischemia of the heart. In the case of the migrainous variety of angina, the symptoms can sometimes appear completely confirmed to that on the EKG. One should not think that if the ECG looks okay, the person has no angina. It is because the changes in the ECG finding ischemia might last just for a short time.
An exercise stress test is a diagnosis approach that consists of a treadmill or bicycle exercise of the patient under continuous ECG monitoring, the measurement of the blood pressure, and also the checking of whether the patient has no pain or chest pain. The forces are being supplemented to trigger the heart to begin ischemic symptoms. Both ECG modifications, as well as angina, or a deviation from the expected blood pressure, are warnings of serious traffic reduction in coronary vessels. In these cases, a patient can undergo a pharmacologic stress test with medications such as adenosine or dobutamine.
Myocardial perfusion imaging scans in the myocardium utilize waste material such as technetium with SPECT to demonstrate blood movement to the heart muscle under two conditions: while the person is at rest and during stress. Changeable perfusion deformities are the results of inducible ischemia and the fixed ones indicate the old infarction.
It increases diagnostic accuracy in those patients whose stress ECG is equivocal and eliminates the problem of guessing myocardial ischemic injury by count. The more advanced technique, the PET imaging method, allows for the possibility of blood flow measurements, myocardial muscle thickness, and multiple vessel disease detection thanks to being of high resolution.
Coronary angiography continues to be the best method for the evaluation of coronary anatomy. It's the same procedure that consists of inserting a catheter into a coronary ostium. This is succeeded by kissing a contrast agent with the help of a fluoroscope in order to diagnose stenoses. These procedures locate the exact place and the degree of the stenosis and thus can perform both revascularization.
Apart from that FFR and IVUS can be used in addition to further measure the severity of the lesion. Nevertheless, angiography carries some risks of bleeding, vascular injury, contrast nephropathy, and arrhythmias, thus patient selection is very important.
Cardiac computed tomography angiography (CCTA) is a non-invasive radiological test. It shows the heart and the coronary arteries by use of a contrast-enhanced CT scanner. That detects both kinds of plagues, which are calcified and noncalcified. It also gives an estimate of the severity of the stenosis. Patients who have a low to moderate risk before testing and CT results that show no presence of the disease can be diagnosed as having no significant problem with CAS about their disease.
Biomarkers, such as troponin I or T and creatine kinase-MB, are quite valuable assets in the diagnosis of acute coronary syndromes. However, they will not be of any significance in the case of pure stable angina. The higher concentration of the above-mentioned substances marks the end of myocardial tissue and triggers unstable angina, leading to a cardiac necrotic infarction. The most sensitive troponin test can detect minor damage soon.
The accuracy of the measurement time is quite crucial. It is because, at that time, the early measurements may bring out a negative outcome, which is a false one. Further experimental biomarkers that are specifically targeted at inflammation or plaque instability are in the course of study, but still, they are not a part of the evaluation of the angina problem that is routine.
Angina treatment is mainly for the relief of the symptoms, bettering the life quality, and reducing cardiovascular events. In the case of patients with stable angina, doctors start by making changes to their lifestyles and taking medications. They, however, keep an operation for the unresponsive cases or the ones that are regarded as the most susceptible.
Angina treatment engagements should be anchored on lifestyle modification. Patients receive information on the foods that form a good diet rich in fruits, vegetables, whole grains, and lean proteins and the ones to be avoided such as saturated fats, excessive salt, and processed foods. On the other hand, moderate regular exercise is good for cardiovascular fitness and endothelial health. It can be beneficial in illness prevention.
It is recommended that one person should have at least 150 minutes of moderate-intensity aerobic activity a week. This can be changed in accordance with the feasible for each individual. Reduction of anxiety, via counseling or mindfulness, and understanding personal strengths, together with coping skills to managing emotional challenges, may significantly decrease overactivity and thus improve mental well-being.
Consequently, with the non-treatment of diseases, revascularization therapy may be used or diagnosed by performing the tests and judgments by analyzing these medical conditions. A percutaneous coronary intervention (PCI) finishes the stenosis procedure by inserting a stent and opening the occluded vessel. Drug-eluting stents stop the coronary from narrowing, but dual antiplatelet therapy has the potential to interact for a long time, thus leading to the risk of bleeding.
Enhanced external counterpulsation (a treatment approach with a different health professional) has been found to be a reliable, completely non-invasive alternative for stubborn angina that does not allow for a PCI. It is the use of air pressure that changes every few seconds if a patient recently had a heart procedure or if the heart is not working well.
It facilitates coronary artery perfusion in diastole and by reducing the left ventricular burden it has cardioprotective effects. Usually, there are about 35 sessions of the given procedure and the patient does one session every day but for seven weeks. If an individual is to benefit from such a treatment, then there are multiple factors to be expected. Therefore, an essential understanding of the patient's issues so that an effective selection can be made.
Table of Contents