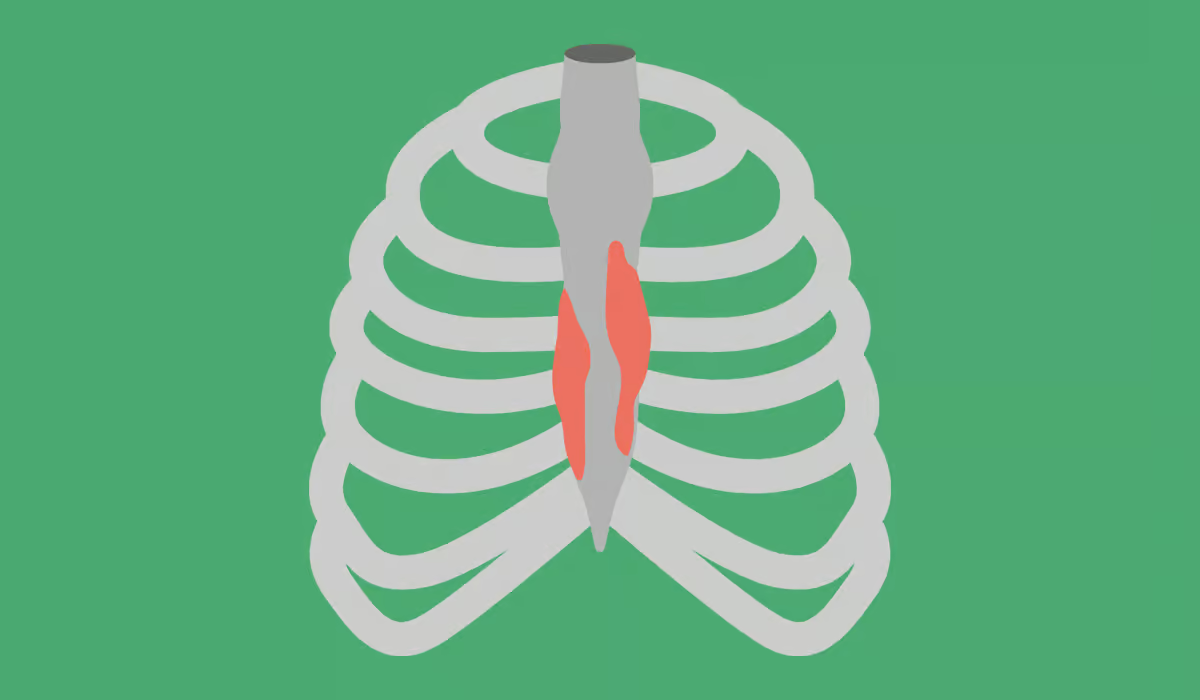
Costochondritis is a condition that is caused by inflammation of the cartilage that surrounds the rib and is attached to the breastbone. This place where it meets is called the costosternal joint, and when it is inflamed, it can result in the sensation of severe, cutting, slit, or pressure-like chest pain. Usually, pain in costochondritis is limited to the front of your chest. However, it can also…
Table of Contents