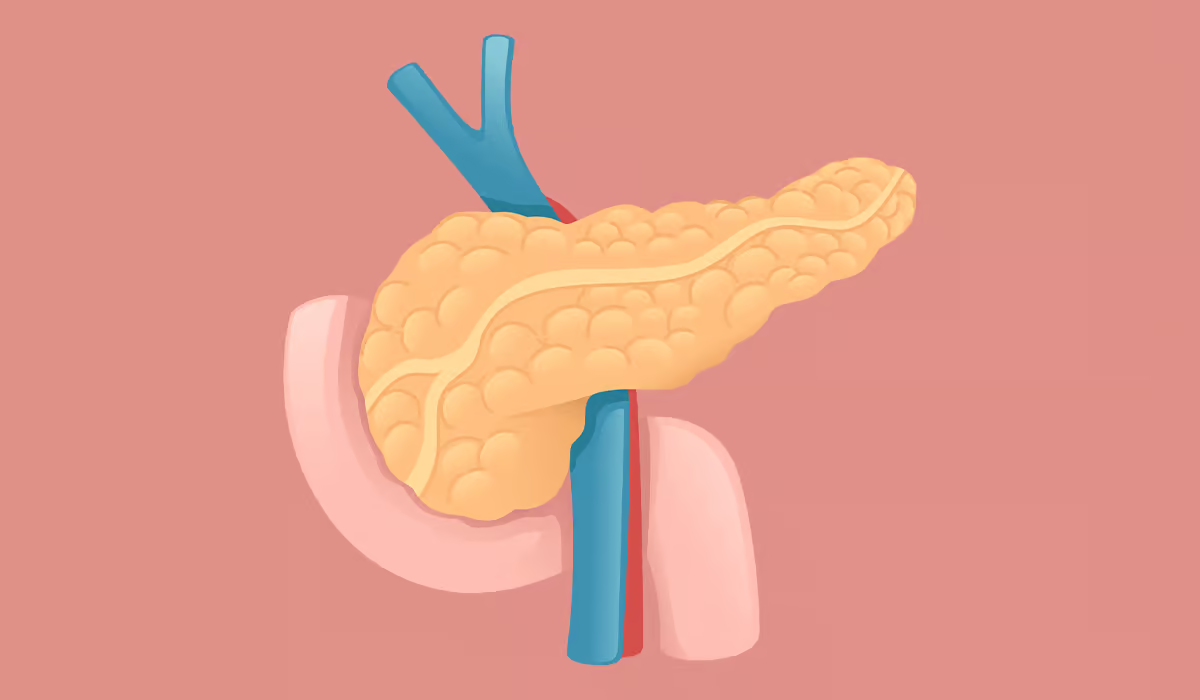
This extraordinary organ governs a lot of valuable functions in the human body. It changes how sugars are processed and produces pancreatic enzymes responsible for digesting proteins or fats. But this gland gets inflamed at times, and its functions get broked.
There are two main types of pancreas inflammation: acute and chronic. Acute pancreatitis is an acute disease that can take a very rapid course. Acute pancreatitis is one of the more commonly treated gastrointestinal ailments that cause hospital admissions in the USA.
Generally, the clinical course of the disease is mild to moderate in intensity in most pancreatitis patients. In contrast, chronic pancreatitis is a disease of optical fibroinflammation. This has not been as swift an evolvement as acute pancreatitis, but it can still cause progressive impairment in gland function. There are several reasons why things can go into an acute or chronic inflammation state. The diseased organ can have varying intensity and character of symptoms.
Pancreatitis is not a simple condition. Diagnosis and stratification by intensity—which has implications for appropriate management—should be prompt. The care of acute pancreatitis cannot be discussed without emphasizing fluid management, diet support, and strategies to reduce risk. Since untreated pancreatitis can damage pancreatic cells, which can lead to serious problems, correct diagnosis and initiation of treatment are crucial. Get the details on this frequent pancreatic condition.
From a biological point of view, pancreatitis is the result of digestive enzymes made by this organ activating in inappropriate circumstances. These enzymes are activated when they are still in the organ, not when secreted into the small intestine. This can happen if the pancreatic duct is inflamed or blocked. The duct is where the enzymes flow to the intestines from the pancreas. Destruction and loss of functional pancreatic tissue, along with duct obstruction, compel loss of organ function in the setting of chronic inflammation combined with frequent episodes of inflammation.
In contrast, it has been claimed that acute pancreatitis has a more brisk and fulminant clinical course in which a pan-systemic immune response of extreme can show and initiate organ failure. Pancreatitis is an inflammatory process of the pancreas caused by pancreatic parenchymal injury. Disease intensity is determined by the volume of damaged pancreatic parenchyma, as well as the strength and type of immune response that follows.
There are many reasons why this balance of the organ can be upset. Now, let us review what causes pancreatitis most frequently.
Also, smoking and drinking alcohol aggravate acute pancreatitis and provoke systemic inflammatory response syndrome. Hence, it can be said that smoking and alcohol-drinking habits are determined risk factors for pancreatic diseases.

Alcohol, cigarette smoking, and other unhealthy habits all perturb the adaptive immune system and additionally elevate pancreatitis risk. The classical form of alcohol- or cigarette-smoking-associated chronic pancreatitis starts as recurrent painful attacks of pancreatitis and grinds down to a chronic, insidious, and debilitating disease. This kind of case usually develops for years after the first isolation. It doesn't sound very good.
The genetic component of the pathogenesis of pancreatitis Some mutations in these genes have been implicated in the excess susceptibility to this inflammatory disease, researchers said. Hence, it follows that some at-risk genetic family members are unaffected by the fact that they were born vulnerable to some disease. Hereditary pancreatitis is a rare autosomal disorder.
Hence, genetic testing for hereditary pancreatitis should be performed in patients with ongoing acute pancreatitis and chronic pancreatitis that have been around for many years. In many of these cases, they present as seemingly idiopathic early-onset pancreatitis.
Certain medications may have a higher possibility of developing pancreatitis. Drugs of this sort include medications that are employed for Crohn's disease. Pancreatitis is reported as an adverse event of treatment. An estimated risk of pancreatitis overall in users of these drugs exists, but the likelihood is minimal. This suggests that in patients who experienced inflammation due to the drugs, cases were mild and reversible upon drug discontinuation. But this is why you should always read the package inserts with pills.
Cholecystitis (gallstones) produces symptoms and problems. Do you know what this disease is? The disease mechanism consists of insoluble biological deposits of chemicals in the gallbladder and bile ducts. One of the top triggers of acute pancreatitis is gallstones. Gallstones from the gallbladder can travel and become lodged in the pancreatic duct. These gallstones land then, block the duct, and cause inflammation.

Viral infections are unpleasant diseases that sometimes have adverse consequences. Infections can also cause a pathological condition of the organ. Plus, infections—that is, viral hepatitis—could cause acute pancreatitis. The infection can travel to the pancreas and create swelling there. Mononucleosis can also be an extremely uncommon complication of mononucleosis. Mostly asymptomatic, EBV infection may lead to more intense problems on rarer occasions.
It's not a very good sign when patients have high lipid levels. Extremely elevated triglyceride level ≤ 1,000 mg/dl is a well-known risk factor for acute pancreatitis. Triglycerides may thus stem from the fatty tissue surrounding the gland parenchyma and from within the gland. Triglycerides are also metabolized in the blood, often raised in acute pancreatitis.
You might think calcium should be a good thing that you can never get too much of. Deficiencies should be avoided, but — sad to say — even excess is not good. Too much calcium in the body is called hypercalcemia. It's not common — but it can happen. This varies from mild to severe symptomatology depending on the calcium concentration, which may be moderate or serious.
Acute pancreatitis can be a problem of severe hypercalcemia. The pancreatic proenzymes have a unique relationship wherein when calcium is present, the proenzymes become activated – only to culminate in gallstones and acute inflammation of the gland.

Tumors — either cancerous or not — can also press on the organ. Obstructing the pancreatic duct by peripancreatic tumors, pancreatic head mass, and cystic lesions of the pancreas may also cause inadequate flow of enzymes, leading to appropriate activation of enzymes in the organ. Pancreatic strictures can also obstruct the pancreatic duct and induce inflammation, an additional problem.
Chronic inflammation results in scarring and fibrosis of the ducts and thus permanent damage to many structures, creating dysfunction of their secretory functions, exocrine and endocrine. Now, let us give you an example: the patients become pancreatic insufficient because of the impaired exocrine function, which leads to a different manifestation. This is a critical situation where more than 90% of the pancreas has been damaged, and it is called pancreatic insufficiency. And so the organ does not function well. In addition, it portends systemic ailments due to endocrine dysfunction entailed by pancreatic diseases.
As with acute pancreatitis, this differs from chronic obstruction. Chronic pancreatitis may remain asymptomatic for a long time. If they appear at all, symptoms are less severe during chronic inflammation. Acute inflammation complaints come on suddenly and strongly. There are other ways that the chronic disease process differs from acute pancreatitis. This means we need to view the changes in the body at a more detailed level — histologically — as the nature of the inflammatory cells present is different. What are the symptoms when the pancreas cries out for help? See for yourself.
One of the frequently occurring symptoms when there are disorders in the pancreas is abdominal pain. And I'm sure you can relate to when your stomach is hurting. It can happen following an overly decadent meal. It's like this: that's how you feel then. The pain can only be a lot more intense and unwanted in acute inflammation. Acute disease is characterized by sudden belly pain. The patient typically presents with epigastric pain that is moderate to severe.
The pain can be referred to the back and seems unbearable. The pain is usually worse after a meal or after the consumption of alcohol. Chronic pancreatitis, in contrast, can present with persistent abdominal discomfort interspersed with intervals of quiescent pain. Also, belly pain can be relieved if you bend forward.

Most missed second symptoms that should ring the bell that maybe, simply possibly, the pancreas is in trouble are nausea and throwing up. Not surprisingly, these are pretty nasty symptoms to have. Acute pancreatitis is usually associated with nausea and throwing up. May vomit often, possibly with bile. Nausea and vomiting — poorer people with chronic conditions may feel sick or vomit, leading to a weight loss as it is hard to eat. Abdominal pain is worsened with vomiting.
Diarrhea is also appreciated in chronic inflammation. This is another symptom that causes the necessity of losing kilograms; patients may appreciate this themselves, but it is a bad sign. Additionally, diarrhea can periodically increase all symptoms of belly pain. Total clinical signs of bowel problems include greasy, smelly, hard-to-flush stools.
Fever is usually not great. Patients have about +38ºC, with severe cases characterized by the development of hypotension. If a patient has a high temperature, we can say about the presence of infection. Sometimes, a viral infection may provoke pancreatitis.
Diabetes-related symptoms are not rare during chronic pancreatitis. Other signs that develop later in the disease process are glucose intolerance or diabetes with pancreatic involvement. This is particularly so for alcohol abuser patients. Patients with poor habits are liable to diabetic phenomena and glucose regulatory disorders. That's because the functions of this organ are directly linked to glucose. Chronic inflammation, in turn, leads to dysfunction of the endocrine pancreas and, finally, pancreatic diabetes.
Only when the patient is well-diagnosed can pancreatitis be treated. Chronic inflammation may start with acute inflammation, and it may end up causing several issues and problems. History, especially of symptoms of gallstones, and inquiry about alcohol abuse are a major component of the first evaluation of suspected acute pancreatitis. Laboratory tests also provide different indications that the organ is not working properly. Also, the imaging check is often useful to see the state of the patient. Learn what tests your doctor will perform.

Laboratory tests for chronic pancreatitis include a complete blood count, among other basic tests. Other essentials include a basic metabolic panel, liver function test, lipid panel, etc. Lipase and amylase levels can be elevated but are often normal in chronic inflammation with pancreatic fibrosis. If yes, then the doctor may not be sure of the results. However, it should be checked that in acute inflammation, lipase or amylase levels are three times higher than the upper limit of normal.
Another important test that is often performed is the quantification of the content of fecal fat. On the other hand, doctors should also carry out genetic exams of kids for cystic fibrosis since it could be an underlying reason. On the other hand, in cases with suspicion of chronic autoimmune pancreatitis, inflammatory markers can be received.
The primary imaging study for diagnosis is magnetic resonance cholangiopancreatography; due to calcifications, these are pathognomonic manifestations that allow the physician to diagnose easily. Pancreatic enlargement, ductal obstruction, or ductal dilatation may also be noted. An alternative that may be performed during the diagnostic procedure is an belly CT scan. It can also exclude other pathologies using a CT scan.
An alternative imaging modality is endoscopic ultrasonography, which may also be used to diagnose the disease. In the early stages of the disease, endoscopic ultrasound provides information about ductal and parenchymal lesions. A chest radiogram is often done in moderate to severe cases to evaluate pleural effusions, which signifies a more advanced disease state and increased mortality. There are many different tests, but they're worth it for a full case review.
Can pancreatitis be treated? It's a very relevant question. Continued alcohol consumption, smoking, and end-stage liver failure are all associated with a poor prognosis. On the other hand, the diseased organ can be cured, but it takes patient commitment, i.e., if the patient follows the treatment course strictly and maintains a healthy diet. Special treatments are needed for both acute and chronic pancreatitis. See what doctors and experts are saying.

Although you might not have heard about it, fluid resuscitation is one of the most important elements in acute pancreatitis. Early aggressive fluid resuscitation is paramount in the management, and lactated Ringer's solution is the fluid of choice if no other contraindications to fluid administration are present. Fluid therapy needs to be done early and as soon as possible. Mortality and complications —Both are lowered owing to fluid therapy.
Fighting pain is one of the most important parts of any treatment that is needed for patients who have suffered from acute inflammation because such people will be going through very harsh and unbearable symptoms of severe pain, which makes it hard to do any activity. Pancreatitis is a sadly painful business. Strego pancreatitis uses non-steroidal anti-inflammatory drugs and powerful opioid painkillers, so it may sound simple. Pain relievers are also used to treat chronic inflammation. However, you should note that these pills are not meant for long-term use.
With just a few exceptions, antibiotics should never be used prophylactically. These powerful medications should be used carefully. Antibiotics are administered for more serious instances, combined with contaminated pancreatic necrosis. In patients with acute pancreatitis in stable condition, drugs are required for weeks. If the therapy with medications does not succeed, surgical treatment of the pancreatic focus is inevitable.
Habits need to be replaced by healthy ones to treat pancreatitis. Additionally, we must still act upon behavior to avoid the presence or worsening of chronic pancreatitis. It asks patients to refrain from drinking and smoking, which is logical since these are possible triggers. The scientist said changing diet can also help. Generally, it is suggested to have small and frequent meals which are low in fat and replacement of fat-soluble vitamins and pancreatic enzymes. Hospital care is also needed for severe cases.

Surgery should be considered in patients failing medical therapy with ongoing pain. As far as gallstones go, it is a no-brainer that the gallbladder must be removed. In other instances, surgery is necessary—the presence of a pancreatic abscess, fistula, or cyst. Surgery is also subjected to tendency due to the presence of pancreatic ascites. Doctors also perform surgery in case of mechanical obstruction of the common bile duct or bleeding. Results of pancreatic resection surgery are acceptable in experienced hands. However, because surgery is invasive, it can be risky as well.
The strategies vary according to the patient's health status affected by pancreatitis. Specific treatment in hypertriglyceridemia seeks to lower the triglycerides levels. Glucose drips are also used. Medium-chain triglycerides also appear to benefit patients, according to data from a novel trial recently reported.
Table of Contents