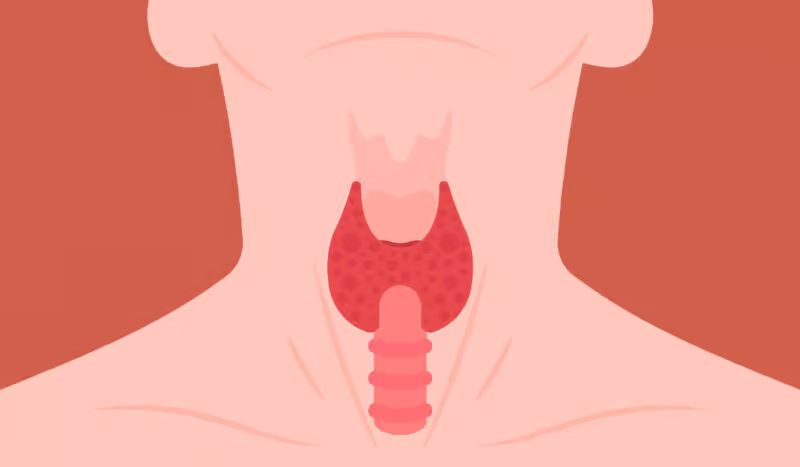
Hashimoto's disease is an autoimmune disorder where the immune system attacks the thyroid gland, leading to... read more »
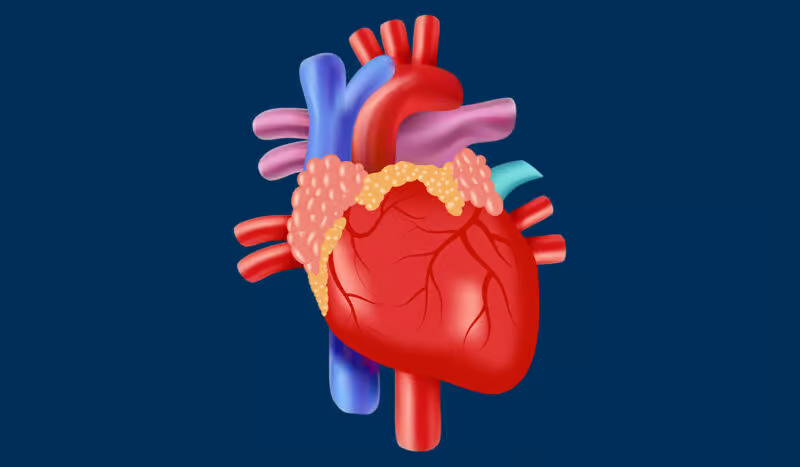
AFib (Atrial Fibrillation) is an irregular, often rapid heart rhythm that can lead to blood clots, stroke, or heart... read more »
An autoimmune disease occurs when the immune system mistakenly attacks the body's own tissues, causing inflammation,... read more »
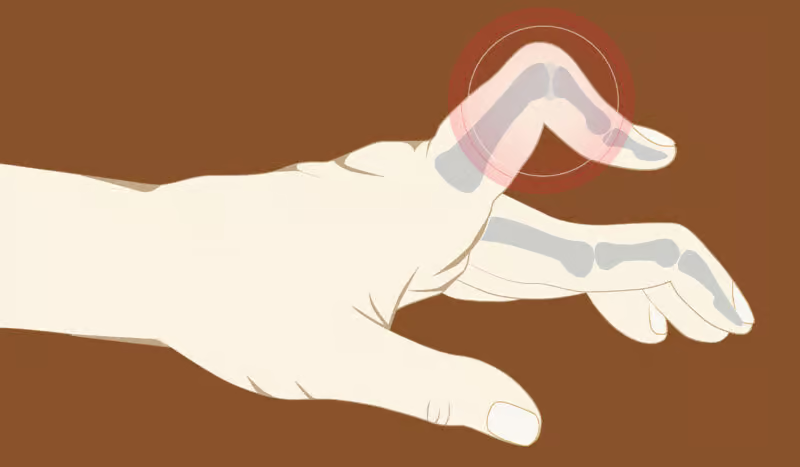
A condition that influences the fingers or the thumb, showing swollen and firm tendons, is known as trigger finger,... read more »
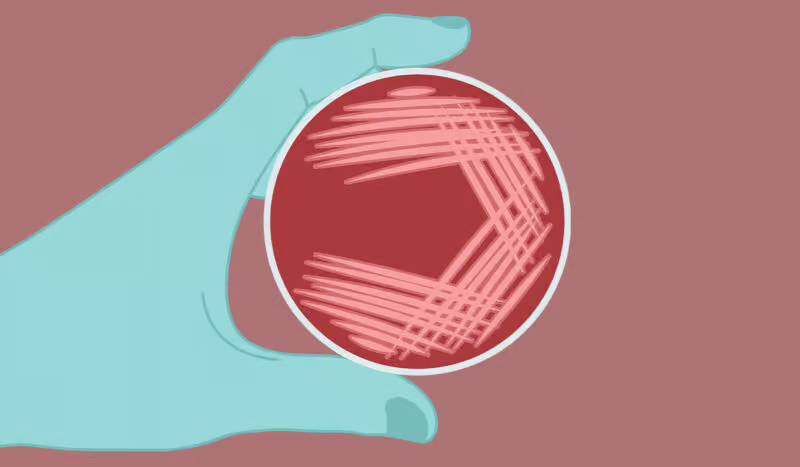
C. Diff is short for the bacteria that causes intestinal infections. The cause of the infection is usually antibiotics.... read more »
Bronchitis is an ailment of the respiratory framework that influences the bronchial tubes, which are the airways that... read more »
Lymphoma is a type of cancer that manipulates the lymphatic system to attack the immune system. The immune system... read more »
Anemia is a condition in which the blood lacks enough healthy red blood cells or hemoglobin, leading to reduced oxygen... read more »
Shingles is a viral infection that occurs after the dormant varicella-zoster virus (VZV) is reactivated. The condition... read more »
Fatty liver is a disease that can result from an unhealthy diet, alcohol abuse and other factors. If left untreated, it... read more »
RSV is a type of virus that causes infections in children and adults. However, children are prone to a more severe... read more »
Neuropathy is nerve damage causing pain, numbness, or weakness, often in the hands and feet, commonly due to diabetes,... read more »
Hemoglobin is a protein in red blood cells that carries oxygen from the lungs to the body and returns carbon dioxide to... read more »
Pancreatitis is a disease that can cause a lot of pain. To avoid serious complications, it is important to get... read more »
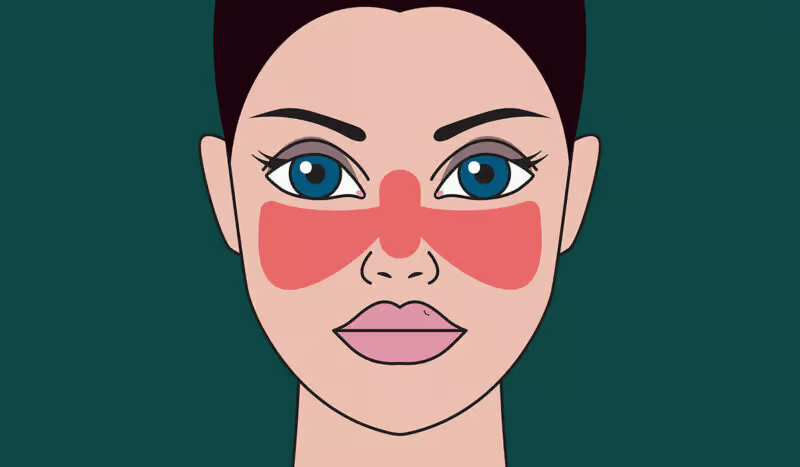
Lupus, a chronic immune system disorder, can be very dangerous to the body of a patient with such a sickness. The... read more »
Sciatica is a type of nerve pain, a nerve that has no parallel within the human body and is caused by pressure,... read more »
Atherosclerosis is a disease that develops over years. Its results can be very dangerous. Read about the signs. Learn... read more »
A gout is an illness that affects the patient, showing them fast and almost unbearable pain. A person is described as... read more »
Bipolar disorder is a mental health condition causing extreme mood swings, including emotional highs (mania) and lows... read more »
Do you know what osteoarthritis is? Here you will find out! We list all the symptoms so you can easily recognize the... read more »
Hemorrhoids, or piles for brief, are the conditions that are caused by the expansion of blood vessels. It occurs within... read more »
Any person of any age can be influenced by hip pain, but it is more serious when it is intolerable to almost not be... read more »
Squamous Cell Carcinoma (SCC) is a skin cancer arising from squamous cells, thin and flat cells in the outer layer of... read more »
Diverticulitis is the inflammation or infection of diverticula, small sac-like structures on the digestive system's... read more »